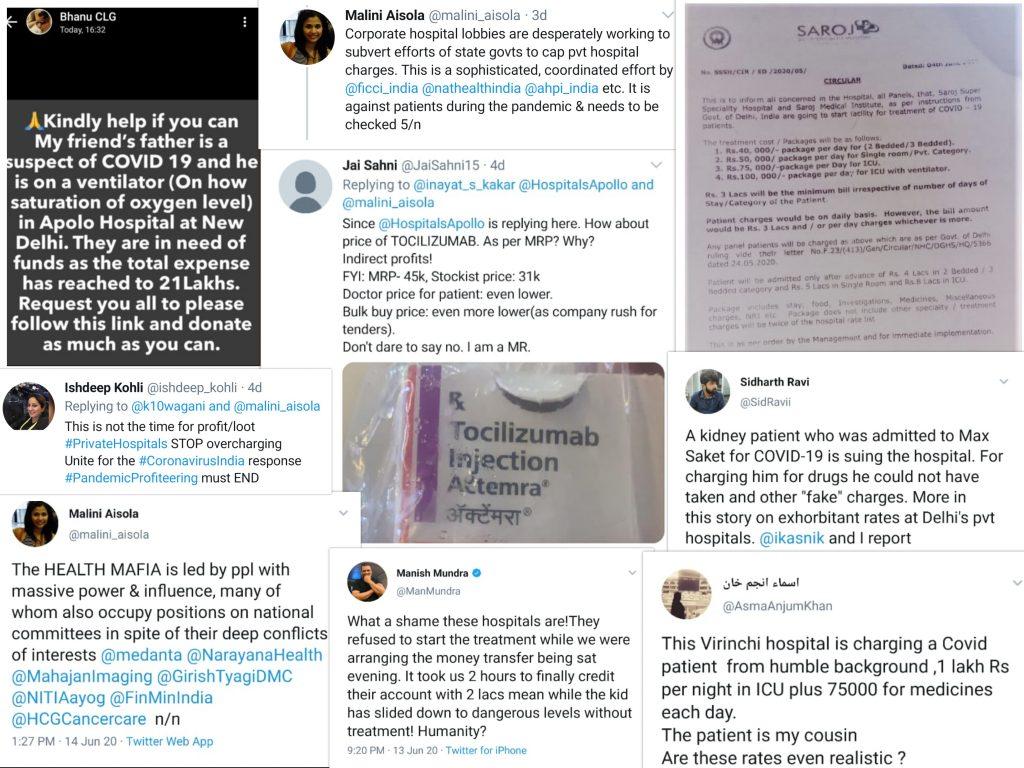
Last week, a “rate” list from a leading for-profit private hospital in Delhi went viral on social media, probably because of the sheer obscenity of the charges that it displayed. The costs for a bed, as per the list, ranged from Rs. 25,000 (about $330) per day in a general ward (no private room, without isolation or ventilator) to Rs. 72,000 (about $950) per day for an ICU bed with ventilator. Given that these rates are grossly unaffordable even by Indian upper-middle class standards, the picture signifies the impossibility of getting affordable quality care for COVID, in India’s capital today. With public hospitals pushed to the brink, COVID patients are being forced to seek private care, and this makes the issue of price regulation critical. A writ petition filed by Advocate Sachin Jain last month in the Supreme Court of India (to which the All India Drug Action Network and the People’s Health Movement (Mumbai) impleaded) is arguing for precisely this.
It is noteworthy that India’s private health sector – one of the largest and most unregulated in the world – was visibly absent in the initial weeks of the COVID pandemic. In April, it was reported that the private sector was handling only one-tenth of the COVID patient load, even though it had two thirds of hospital beds and 80 percent of ventilators in the country. While this was a result of several factors ranging from restrictions placed due to government policy, to “playing it safe”, even in states where no restrictions were placed on private hospitals in treating COVID patients, they remained reluctant to admit such patients. Further, private hospitals also withdrew from providing non-COVID care and this is critical given that a large proportion of healthcare in the country is serviced through private players. In order to correct this, several state governments had to issue special circulars instructing private providers to resume services. As the burden of the COVID response on India’s flailing public health system increases, various state and national governments have called upon private hospitals to deliver care.
Unaffordable costs for COVID care
Cost regulation, however, has remained contentious – while in some states the government is providing free treatment in requisitioned private hospitals by reimbursing them at fixed package rates (West Bengal), and states such as Maharashtra have capped prices on treatment, in others, like Delhi, select private hospitals have been designated to provide COVID-19 treatment without any price regulations. But even in states with price regulation, corporate private hospitals continue to profiteer by charging exorbitant and irrational costs to patients. Components such as high-end medicines, Personal Protective Equipment (PPE), COVID-19 tests, interventional procedures which constitute a significant portion of bills are excluded from the costs capped by governments. For instance, an analysis (by the impleaders) of bills from corporate hospitals in three metropolitan cities shows two distinct ways in which corporate hospital chains are profiteering on PPE- one, patients are being charged inflated costs of PPE; and two, each PPE kit is billed to multiple patients. A common practice which hospitals have used to evade transparency is to bill PPE as a per day cost, without mentioning the number of PPE kits used or per unit cost of each PPE kit. In their petition to the court, impleaders also note that typically, COVID treatment at present is largely supportive and does not require surgical intervention. Yet, the costs often surpass that of major surgeries. Even patients with private insurance have borne out of pocket expenses, as insurance companies have refused to cover costs of extended duration of hospitalization, PPEs, biomedical waste disposal charges and other requirements for COVID care such as care and hygiene charges, thermometer and handrub. Private insurance companies in India have gone on record to say that private hospitals are charging unnecessarily high costs of care which insurance companies cannot afford to cover.
Increasing costs for non-COVID care
An ignored facet of overcharging during the Covid-19 crisis has been the increase in costs of non-COVID treatment in private hospitals during the pandemic. As the number of cases has risen, more and more government hospitals have been converted entirely into “COVID hospitals”, leaving many non-COVID patients who are dependent on public hospitals (often due to economic reasons) for essential and lifesaving treatments such as chemotherapy, radiation, dialysis, abortion without continued care. Such patients are being forced to access care in private hospitals where costs of treatment have been inflated to make up for the loss of footfall. Private hospitals have been forcing patients to deposit hefty sums of money (approx USD 2600-3,900) in order to gain access to non- Covid treatment. These deposits act as financial barriers to people in need of essential care. There have been instances where private hospitals have compelled non-Covid patients to pay for a Covid-19 test in order to access services, even in cases where national testing guidelines do not permit a Covid test to be conducted. As an example, a dialysis dependent patient was forced to pay more than 15 times the cost of dialysis treatment in a private facility as the hospital insisted on doing the dialysis only in the ICU.
Response of the Union Government
As the number of cases rise in the country, and more hospitalization is envisaged, the question of costs is likely to become a significant one for patients seeking care, making this writ petition a very significant and timely one. The response of the Union Government in Court, however, suggests that it is not keen to regulate private hospitals. It has argued in the Supreme Court that under the Ayushman Bharat Prime Minister’s Jan Arogya Yojana (AB-PMJAY) scheme which seeks to ‘to mitigate the adverse impact of this catastrophic illness on the poor’, costs would be taken care of, and hence pricing caps are unnecessary. However, data shows that only a fraction of COVID testing and treatment is being provided through the scheme as enrollment is still low, and because the scheme only provides for Rs. 5 lakh (approx. USD 6500) coverage for the entire family – an amount far less than some of the costs that have been reported for COVID treatment for a single patient requiring ICU care and ventilator. It has also argued that the Union Government does not have authority to mandate prices for the private health sector and this is in fact the role of the State Governments. However, with the National Disaster Management Act in place, the Union government does have such legislative authority. In general, the responses of the Union Government so far suggest reluctance to take a position on the issue of price ceilings.
Beyond price regulation
Over the past several years, private sector engagement (PSE) is increasingly gaining ground, both within global health policy circles and national health policy making. Strengthening PSE has been flagged as one of the key pathways to achieving Universal Health Coverage, and more recently a coordinated and comprehensive response to the COVID pandemic by the WHO. Indeed, several countries globally have been able to effectively involve and regulate the private sector during the pandemic. However, the way that the private sector has acted in India during the COVID pandemic, holds lessons for both global health policy as well as national health policy, on what regulatory frameworks are needed to truly harness any potential that the sector has, and the State’s capacity (and intent) to enforce such regulation. While this article deals only with the issue of pricing in large corporate hospitals, there is a whole diversity of providers who may have different concerns and this needs exploration. Some experts have argued that it is not capping of prices, but in fact “competition” that will truly regulate the private providers. But if there is one thing that the COVID pandemic has made clear, it is that “the market never regulates healthcare in the public interest”; it is the state that must do so. At a truly existential moment, the private health sector has failed to either act rationally or equitably. That said, however, price capping is by no means the only way to address regulation of the private sector and Indian health care more broadly. Most critically, what we have seen in India over the past three months is the deplorable state of its public health services; had the public sector been well-functioning, for-profit private players would not have been able to profiteer in this manner. If this opportunity is not harnessed, we may go back to allowing a predatory private sector to continue functioning as usual, without regard to health as a public good.
Opinions expressed in this article are personal and do not necessarily reflect the position of the groups to which the authors belong.